


ER Editor: UPDATE — here is Dr. Jessica Rose’s response to Rancourt’s work
Denis Rancourt (and team’s) new report on vaccine dose fatality rate (vDFR) – in a nutshell
***
We highly recommend the work of Canadian researcher Dr. Denis Rancourt. A couple of relevant tweets from him first:
In our new article, which will be posted this week, we estimate that ❗️13 MILLION❗️ were killed by the COVID-19 vaccines to date, worldwide.
The great majority old and frail.
The number for India alone is 3.7 million.
All-cause mortality is a powerful information source.— Denis Rancourt (@denisrancourt) February 8, 2023
Here it is! The first rigorous vaccine toxicity measurements by age, goes exponential with age, >300K deaths USA, 13M deaths global. pic.twitter.com/x7vuVT0qcW
— Denis Rancourt (@denisrancourt) February 9, 2023
Here is the link to Rancourt’s paper at ResearchGate:
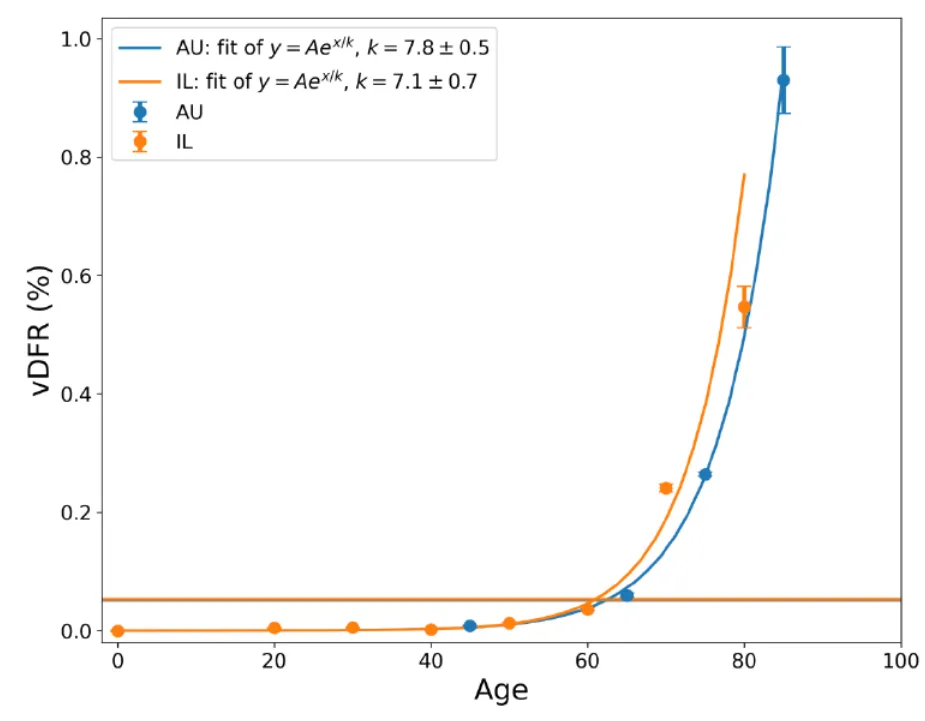
Age-stratified COVID-19 vaccine-dose fatality rate for Israel and Australia
Nice to have my interview with @RobertKennedyJr featured in Suzanne Burdick’s article at @ChildrensHD https://t.co/YVSd4zg9gx
— Denis Rancourt (@denisrancourt) February 10, 2023
Below are ‘takes’ from Dr. Paul Alexander and Steve Kirsch.
This is substacker Peter Halligan‘s interpretation (delivered by e-mail to subscribers):
Good news! Only 13 million dead from C19 injections, implying a URF of 26 and not 40 for reports of death to VAERS and EUDRA – early estimates of a URF of 70 for EUDRA combined with 4-5 times the fatality rate amongst viral vector compared to mRNA injections replaced with identical 1 in 1,000 dose fatality rate from 13 billion doses administered globally from any type of injection!
In our opinion, on a glance at the graph featured in Steve Kirsch’s piece, it looks like the vaccine, along with malicious carehome policies (shipping the elderly out of hospitals into carehomes, denuding these places of staff, putting the elderly on Do Not Resuscitate notices, ‘treating’ them with end-of-life shots such as Midazolam, denying food and water, etc.) plus ‘we’re protecting the elderly – roll up first to get your shot’ media-propaganda appeals, were all a ploy to bump off as many of them as possible.
********
Shocking (yet we told them so) age-stratified COVID-19 vaccine-dose fatality rate (vDFR) for Israel & Australia; confirms that COVID gene injections (mRNA-DNA) cause deaths & dramatically in elderly
Rancourt again gives us a glimpse with his team of superb scholarship as he unpacks the age-stratified data, finding that the elderly are at greatest risk of death from vaccine over younger

Firstly, this COVID gene injection, whether mRNA or DNA platform, and as such any of these gene injections that end in the spike protein to build the immune response, MUST be stopped! Immediately. Complete, based on the ‘body of evidence’ that has accumulated on ineffectiveness and harms.
We know from autopsy studies and adverse effect monitoring that the COVID-19 vaccines can cause death. The evidence landscape is now firm that the COVID gene injection (mRNA- or DNA platform) is ineffective, gets to negative effectiveness, drives infection in the vaccinated, drives immune tolerance (IgG class-switch induced antibodies), drives original antigenic sin immune fixation or imprinting (recall antibodies), drives paradoxical priming, drives viral immune escape, drives antibody-dependent enhancement of infection (ADEI) and also of disease (ADED), and drives infectious variants as well as causes deaths across all age-groups administered.
For this examination, vaccine-dose fatality rate (vDFR) is the ratio of vaccine-induced deaths to delivered/administered vaccine doses.
Researchers found that the ‘vDFR increases dramatically with age for older adults, being exponential with a doubling time of approximately 5.2 ± 0.4 years. As a result the vDFR is an order of magnitude greater in the most elderly population than the all-population value, reaching 0.6 % for the 80+ years age group in Israel and 1% for the 85+ years age group in Australia, compared to < 0.01 % for young adults (< 45 year olds).’ The results indicate that it is dangerous and deadly to focus vaccinating (or prioritize) those deemed to be at greatest need of protection.’ This being the elderly.







I have been against these COVID vaccines en toto, day one. We have said that vaccine may be, based on informed consent, risks and benefits properly explained, focused on the high-risk. Yet this data is clearly showing that we are even wrong to administer this to our high-risk precious elderly. They have early treatment available. We know of Vitamin D3 as potent in reducing severity and mortality especially if serum levels remain above 50 to 60. I again state as firmly as I can that all we needed day one in this pandemic and still today is to:
1)isolate and quarantine ONLY sick and unwell persons; never ever isolate well asymptomatic persons in a society or at the border; I do not mean FORCED quarantine, I mean also that unwell persons will take the steps needed as we have always done e.g. a a sick persons typically know they are sick and stays away from work etc. and we were always dealing with a largely benign flu, cold like respiratory ILI pathogen. This was never Nipah or Ebola etc. (Marius reminded me it must never be forced and this has always been the view for THIS pathogen); never ever MASS test asymptomatic persons especially with a process like the RT-PCR that was 95% false-positive being over-cycled beyond 24 cycles that then only detect viral dust and fragments and unculturable non-infectious, non-lethal pathogen
2) you strongly double and triple down protect the vulnerable e.g. elderly and other high-risk persons; this is a key component for any move towards achieving population herd immunity; this is no call to ‘let it rip’; the vulnerable often cannot take vaccine or be exposed directly so we use the low-risk ‘recovered’ population to protect the vulnerable
3)we allow the vast rest of the low-risk, healthy persons, including children, to live freely, unfettered lives, no lockdowns, no school closures, just taking reasonable precautions.
4)use early treatment as needed, used Vitamin D3 lavishly, use nasal-oral rinses, and ventilate homes, and if needed in homes, use oxygen support.
This is the reason why we should not have used the population as guinea pigs to trial these vaccines as to the long-term effects. The data is showing what would have emerged had Pfizer and Moderna been phased properly and to sample size and duration and this data underscores that the regulator FDA failed the American population. Health Canada failed the Canadian population. All such regulators caused deaths to their populations.
You have to bear in mind that the median/mean age of death from end-stage COVID was 82 to 83 years in February 2020 and remains so today February 2023, 3 years out, and with 2-3 underlying medical conditions. Evidence indicates that those over 70 who died in the US had as many as 5 underlying conditions. COVID spared our children unlike seasonal influenza that kills our children and today, the death rate is near zero for children 10 and under and 0.0003% for those 0-19 years. The IFR is settling out to be 0.05% globally ranging I argue and based on superb work by Ioannidis from 0.03 to 0.07% in those up to 70 years. This means that the death rate is at or below seasonal influenza, estimated to be about 0.1%. COVID kills at median of about 82 years while life expectancy is about 79 years. This means that COVID did not cut lives short and killed beyond life expectancy. Bear that in mind.
This is my assessment this morning.

SOURCE:
See also Awakenotwoke substack, please take a look at this good scholarship:
https://substack.com/profile/88409534-awakenotwoke?utm_source=account-card
Source
********
New paper: An estimated 13 million people worldwide killed by the COVID vaccines
That’s twice as many as were killed by the virus. In the US, the estimates are 670K Americans killed. Perhaps it’s time to declare that the vaccines are a worldwide emergency?

Executive summary
The paper suggests you can take the number of vaccine doses delivered, divide by 1,000 to get an estimate of the number of people killed by the COVID vaccine.
The tweet directly from the author sums it up:
The details
The paper: Age-stratified COVID-19 vaccine-dose fatality rate for Israel and Australia
The full story about how universities undermine people like Denis Rancourt who tell the truth
The main result
The paper finds that the vDFR (vaccine-dose fatality rate) is exponential with respect to age.
The paper points out that “it is not unreasonable to assume an all-population global value of vDFR = 0.1 %”
For the US, 670M doses have been given, so the estimate is 670,000 people have been killed by the COVID vaccines in the US.
I have said for a long time that the URF in VAERS is 41, and there are 16,300 excess US deaths in VAERS (subtracting 250 background deaths per year which gets reported into VAERS) which comes to 668K.
668K is very close to 670K, isn’t it?
What an amazing “coincidence”!
Summary
The paper gives a simple way to estimate the number of people a country has killed by deploying the COVID vaccines: 0.001*# of doses.
In short, you can just take the number of vaccine doses in millions and just change “millions” to “thousands” to estimate the number of people killed by the vaccine.
Using data from Israel and Australia, the paper estimates 13 million deaths worldwide from the COVID vaccines:
The COVID-19 vaccines did not only not save lives but they are highly toxic.
On the global scale, given the 3.7 million fatalities in India alone, having vDFR = 1 % (Rancourt, 2022), and given the age-stratified vDFR results presented in this work, it is not unreasonable to assume an all-population global value of vDFR = 0.1 %. Based on the global number of COVID-19 vaccine doses administered to date (13.25 billion 24 doses, up to 24 January 2023, Our World in Data),3 this would correspond to 13 million deaths from the COVID-19 vaccines worldwide. By comparison, the official World Health Organization (WHO) number of COVID-19 deaths to date is 6.8 million (6,817,478 deaths, reported to WHO, as 3 February 2023),4 which are not detected as COVID-19 assignable deaths in ACM studies.
************
Source

••••
The Liberty Beacon Project is now expanding at a near exponential rate, and for this we are grateful and excited! But we must also be practical. For 7 years we have not asked for any donations, and have built this project with our own funds as we grew. We are now experiencing ever increasing growing pains due to the large number of websites and projects we represent. So we have just installed donation buttons on our websites and ask that you consider this when you visit them. Nothing is too small. We thank you for all your support and your considerations … (TLB)
••••
Comment Policy: As a privately owned web site, we reserve the right to remove comments that contain spam, advertising, vulgarity, threats of violence, racism, or personal/abusive attacks on other users. This also applies to trolling, the use of more than one alias, or just intentional mischief. Enforcement of this policy is at the discretion of this websites administrators. Repeat offenders may be blocked or permanently banned without prior warning.
••••
Disclaimer: TLB websites contain copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available to our readers under the provisions of “fair use” in an effort to advance a better understanding of political, health, economic and social issues. The material on this site is distributed without profit to those who have expressed a prior interest in receiving it for research and educational purposes. If you wish to use copyrighted material for purposes other than “fair use” you must request permission from the copyright owner.
••••
Disclaimer: The information and opinions shared are for informational purposes only including, but not limited to, text, graphics, images and other material are not intended as medical advice or instruction. Nothing mentioned is intended to be a substitute for professional medical advice, diagnosis or treatment.



Leave a Reply