MEASLES OUTBREAKS OR A PHILOSOPHY OF DECEPTION?
DR. MIKE WILLIAMS
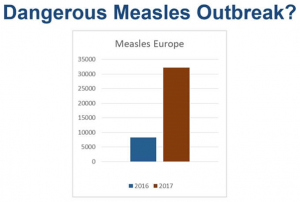
In a prior article, I discussed a recent UK, Bristol Post newspaper story that warned of a measles outbreak and claimed that in Bristol, measles cases were “soaring” and that the “infection [was] now widespread”. I discussed that Measles naturally cycles (goes up and down, predictably) and is endemic in large populations, meaning we can’t eradicate it. Those facts are pretty well understood by anyone who studies epidemiology. UK government data revealed that this current rise in measles cases, contrary to the newspaper’s warning, was actually less than previous rises in the natural cyclical pattern. Hardly, a widespread outbreak.
Articles like that in the Bristol Post are repeated across the globe and misrepresent a natural rise in the predictable cycle of cases consistent with endemic measles as an outbreak that requires every child to be vaccinated immediately, otherwise their lives are in danger. And worse: they generally state that unvaccinated children are the cause of that rise in cases.
Let me be clear: you can vaccinate 100% of children 10 x over, and still you will get measles cases – periodically increasing and decreasing – because that’s what endemic diseases do, and vaccination cannot stop that.
You can see by the Bristol Live’s dramatic picture and comment on the Bristol Mums and Dads Facebook page the kind of effect such an article has.

To anyone with any experience of infectious disease or just a modicum of common sense, however, it was pretty obvious that the photo looked wrong – faked. It was only a matter of time before that was found out.
Here’s the original undoctored photo of the baby, as seen on a Nursing website.

SOURCE: NURSING JOBS
Oh, dear! I think that’s called fake news.
Incredible, how can they do that? I hear you say. Well, that wasn’t the only deceit. I also covered an openDemocracy article that warned of EU citizens’ hesitancy around vaccination and a measles outbreak. The message could be interpreted thus: unvaccinated children are the cause of outbreaks, and if we all got vaccinated, the outbreaks would stop. I highlighted some data the author of that piece hadn’t told you about, easily understood in just two graphs.

The newspaper photoshopped image and the openDemocracy article are sadly just two more examples of a long history of misrepresenting, deceiving and simply lying about the data.
Here is another one. I’ve chosen some extracts from academic papers to highlight the level of subterfuge with vaccine programs.
Burton et al. in WHO and UNICEF estimates of national infant immunization coverage: methods and processes pointed out historical, major problems with gathering data to monitor vaccination programs:
One perceived weakness of the estimates stems from the subjective nature of the methods used… Subjectivity arises primarily in (i) the choice of rules and (ii) deciding which rule should apply in a given circumstance. We have no theoretical foundation for selecting rules and no validation of their reliability; the choices have been based on appeals to rationality, consistency and the lack of alternatives that produce more reasonable estimates. [My emphasis].
They continued:
However, as described in the section above, both methods [of measuring vaccine coverage] are subject to biases. In some instances, these may be identified and corrected, as we have attempted to do. In no instance do we have complete, consistent, multiple measures for an entire country/vaccine time series. In some instances we have complete administrative data validated by periodic or occasional consistent survey findings. In others, data are available from a single source – usually administrative data – and appear internally consistent over time and across vaccines. In several countries, administrative data and survey results are inconsistent;42,43 in others, the administrative time series is incomplete, internally inconsistent or both.40 [My emphasis].
Now let’s hear from a highly respected Global Health researcher and, previously, WHO coordinator for the Health Statistics and Evidence Unit, Dr Kenji Shibuya, who succinctly pointed out the glaring problems with the data gathering and analysis being used to monitor vaccine programs, including measles in Africa:
Dr. Kenji Shibuya
Faculty Chair, GLP Professor, Global Health Policy The University of Tokyo
Dr. Kenji Shibuya is a professor at The University of Tokyo’s Graduate School of Medicine. After teaching at medical schools in Tokyo, Dr. Shibuya joined WHO in 2001 and was coordinator for the Health Statistics and Evidence Unit from 2005 until 2008 when he was appointed at the University of Tokyo. He has been a regular contributor to the World Health Reports and has published widely on issues including mortality, risk factors and health system performance assessment. Dr. Shibuya obtained his MD from The University of Tokyo and PhD in public health from Harvard University.

He stated:
For monitoring, it is important to distinguish between corrected and predicted statistics.3 Corrected statistics use adjustments made for known biases. Predicted statistics use a set of assumptions about the association between other factors and the quantity of interest, such as maternal mortality, to fill gaps in the data over time or space (from one population with data to another with limited or no data). Predicted statistics are useful for planning, decision-making, advocacy for funds and research and development investments when corrected statistics are not available. But they are not suitable for monitoring progress on what works and what does not.3 Unfortunately, the MDG monitoring process relies heavily on predicted statistics.
He continued:
The same applies to monitoring progress in major disease interventions. For example, the assessment of a recent change in measles mortality from vaccination is mostly based on statistics predicted from a set of covariates such as the number of live births, vaccine coverage, vaccine effectiveness and case fatality ratios.4 It is understandable that estimating causes of death over time is a difficult task. However, that is no reason for us to avoid measuring it when we can also measure the quantity of interest directly;5 otherwise the global health community would continue to monitor progress on a spreadsheet with limited empirical basis. This is simply not acceptable. [My emphasis].
In simple terms: Dr Shiuya was stating that any claims about those vaccination programs were derived from statistically manipulated guesswork, not accurately measured data. And no matter how long they sat at their computers and crunched their theoretical numbers of “vaccine effectiveness” and “case fatality ratios” on their excel spreadsheets, they were closer to theoretical fiction than factual reality.
But did government officials, media and trusted international and global organisations tell you that?
This is how they represented the measles data:

SOURCE: UNICEF Measles deaths in Africa plunge by 91 per cent
MEASLES DEATHS IN AFRICA PLUNGE BY 91 PERCENT
“This is a major public health success and a tribute to the commitment of countries in the African region,” said Dr. Margaret Chan, WHO Director-General. “We need to sustain this success and intensify our efforts in other parts of the world, as there are still far too many lives lost to this disease.”
Really? Based on statistics that are not suitable for monitoring progress on what works and what does not?
You’d be forgiven for thinking that you simply could not make this up……But they did! Effectively, a conjured up figure of vaccine success that simply wasn’t true. How could they do that?
In closing
So who do we trust? Is it any wonder, when we see such evidence, that we simply do not trust authority? Are we surprised after reading what Dr Shubiya stated or seeing a faked, photoshopped image of a baby that people are simply fed up with being told how bad they are for not vaccinating their children, and how successful vaccination is. And fed up with being told that any doctor or researcher that simply questions those assumptions, after reading the literature, is a quack. There are serious, glaring and obvious problems with vaccination, some pointed out here. And the push for an authoritarian model of healthcare with mandatory vaccination at its centre, based on that “evidence”, is deeply flawed and deeply troubling, not least for its lack of credibility but also (as is widely published now) with the rise in morbidity and mortality associated with vaccination, the dangers, potential and otherwise, of its philosophy of deception.
••••
Contributed to TLB Project by author, Dr. Mike Williams
••••
Click on the links or images below to read more great articles by Dr. Mike Williams:
Measles and The “Noble Lie” – By Dr. Mike Williams
No TIME to Die – By Dr. Mike Williams
DISEASE X OR VACCINE X? CHOOSE YOUR POISON
openDemocracy or Measles Conspiracy

••••
The Liberty Beacon Project is now expanding at a near exponential rate, and for this we are grateful and excited! But we must also be practical. For 7 years we have not asked for any donations, and have built this project with our own funds as we grew. We are now experiencing ever increasing growing pains due to the large number of websites and projects we represent. So we have just installed donation buttons on our websites and ask that you consider this when you visit them. Nothing is too small. We thank you for all your support and your considerations … TLB
••••
Click on the image below to visit TLB Project on twitter …